
Quick Answer
An RNP antibody level of 0.2 indicates a low but notable presence of ribonucleoprotein antibodies, which may suggest early or mild immune activity related to autoimmune diseases like mixed connective tissue disease or lupus. This value alone is not diagnostic but warrants further clinical evaluation.
Infobox: RNP Antibodies at 0.2
| Parameter | Details |
|---|---|
| Antibody Type | Ribonucleoprotein (RNP) antibodies |
| Measured Level | 0.2 (unit varies by lab) |
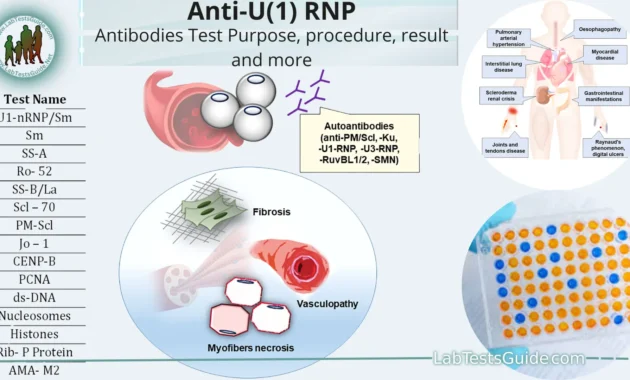
| Associated Conditions | Mixed connective tissue disease (MCTD), systemic lupus erythematosus (SLE) |
| Interpretation | Low positive or borderline; requires clinical correlation |
| Reference Range | Varies by laboratory; often <0.2 considered negative |
| Next Steps | Additional serological tests, clinical assessment, imaging if indicated |
Overview of RNP Antibodies
Ribonucleoprotein (RNP) antibodies are immune proteins that target specific complexes within the cell nucleus. Their presence is commonly linked to autoimmune disorders, particularly mixed connective tissue disease (MCTD) and systemic lupus erythematosus (SLE). These antibodies serve as important biomarkers, helping clinicians understand immune system activity and potential autoimmune pathology.
Clinical Significance of a 0.2 RNP Antibody Level
A measurement of 0.2 for RNP antibodies represents a borderline or low-positive result. While this value does not confirm an autoimmune diagnosis, it signals a subtle immune response that may precede or accompany autoimmune conditions. Interpretation depends heavily on the patient’s symptoms, medical history, and other laboratory findings.
Because reference ranges differ among laboratories, a 0.2 reading might be considered normal in some settings and mildly elevated in others. This variability necessitates a personalized approach to diagnosis and management.
Why Understanding RNP Antibody Levels Matters
Recognizing the implications of RNP antibody levels is crucial for early detection and management of autoimmune diseases. Even a low-level positive result like 0.2 can prompt further investigation, potentially leading to timely intervention and improved patient outcomes. It also helps avoid misdiagnosis by contextualizing laboratory data within the broader clinical picture.
Common Misconceptions About RNP Antibody Results
Myth: A low RNP antibody level definitively means no autoimmune disease.
Fact: Low levels can still be clinically relevant and warrant monitoring.
Myth: All labs use the same reference ranges.
Fact: Reference values vary, so results must be interpreted in context.
Myth: RNP antibodies only appear in severe disease.
Fact: They can be present in mild or early stages as well.
Example Scenario
Consider a patient presenting with joint pain and fatigue. Their RNP antibody test returns a value of 0.2. While this does not confirm an autoimmune disorder, the clinician orders additional tests and reviews symptoms carefully. Over time, if symptoms progress and antibody levels rise, a diagnosis such as mixed connective tissue disease may be established, guiding appropriate treatment.
Related Terms
- Autoimmune Disease: Conditions where the immune system attacks the body’s own tissues.
- Mixed Connective Tissue Disease (MCTD): An autoimmune disorder characterized by features of lupus, scleroderma, and polymyositis.
- Systemic Lupus Erythematosus (SLE): A chronic autoimmune disease affecting multiple organs.
- Serological Tests: Blood tests that detect antibodies or antigens.
Frequently Asked Questions (FAQ)
- What does an RNP antibody level of 0.2 indicate?
- It suggests a low or borderline presence of RNP antibodies, which may or may not be clinically significant depending on symptoms and other findings.
- Can a 0.2 RNP antibody level diagnose an autoimmune disease?
- No, diagnosis requires a combination of clinical evaluation, symptoms, and additional tests.
- Are RNP antibody levels consistent across different labs?
- No, reference ranges vary, so results should be interpreted in the context of the specific laboratory standards.
- Should I be concerned if my RNP antibody level is 0.2 but I have no symptoms?
- Not necessarily, but it is advisable to monitor and consult a healthcare provider for personalized advice.
Final Answer
An RNP antibody level of 0.2 represents a borderline or low-positive finding that alone does not confirm autoimmune disease but signals the need for further clinical assessment. Interpretation depends on individual symptoms, laboratory standards, and additional diagnostic workup to guide appropriate management.
References
- Aringer M, et al. “2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus.” Arthritis Rheumatol. 2019.
- Sharp GC, et al. “Mixed connective tissue disease-an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA).” Am J Med. 1972.
- Petri M. “Review of classification criteria for systemic lupus erythematosus.” Rheum Dis Clin North Am. 2005.
- Laboratory Reference Ranges for Autoimmune Serology. Mayo Clinic Laboratories.




Edward_Philips offers a thoughtful exploration of the nuanced role RNP antibody levels play in diagnosing autoimmune conditions. The value of 0.2, while modest, is not to be dismissed-it represents a subtle yet meaningful signal within the complex immune dialogue. This level acts as a critical hint, prompting clinicians to contextualize results with the patient’s symptoms, history, and additional diagnostic tests. As highlighted, autoimmune markers like RNP antibodies do not exist in isolation; variability in lab reference ranges and individual health backgrounds add layers of complexity. Ultimately, this careful interpretation encourages a holistic, patient-centered approach, emphasizing that even low antibody titers can be integral pieces of a larger clinical puzzle. Edward’s narrative underscores the delicate balance between numbers and nuanced clinical judgment in understanding autoimmune health.
Edward_Philips eloquently captures the intricate significance behind an RNP antibody level of 0.2, highlighting how such a seemingly subtle finding can carry substantial implications in the realm of autoimmune diagnostics. This value acts as an early signal, a prompt to clinicians to consider the broader context-symptoms, medical history, and complementary tests-rather than focusing solely on the numerical result. The discussion importantly emphasizes that RNP antibodies exist within a spectrum, influenced by individual variability and differing laboratory standards. This nuanced perspective reminds us that autoimmune conditions often require a multifaceted investigative approach, where even low-level antibody presence may hint at evolving pathology or risk. In essence, Edward’s thoughtful reflection advocates for vigilance and comprehensive evaluation, turning what might be perceived as a minor lab value into an opportunity for deeper clinical insight and personalized patient care.
Edward_Philips provides a compelling and insightful analysis into the layered meaning behind an RNP antibody level of 0.2. This commentary beautifully illustrates that such a measurement is far from a simple data point; it is a subtle signal demanding careful interpretation within the broader clinical context. By emphasizing the variability among individuals and laboratory standards, Edward reminds us that autoimmune diagnostics require more than episodic snapshots-they require thoughtful synthesis of lab data, symptoms, and medical history. The metaphor of twilight captures the ambiguity of this antibody level perfectly, highlighting its potential as an early indicator rather than a definitive diagnosis. This perspective enriches our understanding, advocating for a vigilant yet measured approach that recognizes the complexity of immune system dynamics and encourages proactive, personalized investigation rather than premature conclusions.
Edward_Philips beautifully elucidates how an RNP antibody level of 0.2 functions as more than just a numerical value-it is an interpretive gateway into the complexities of immune health. This level, subtle yet meaningful, underscores the importance of integrating lab results with clinical context, including patient history and symptomatology. As Edward highlights, autoimmune diagnostics cannot rely on solitary data points but require a comprehensive, patient-specific investigation to unravel the underlying immunological narrative. His metaphor of a “soft glow of twilight” aptly conveys the ambiguity and potential significance of this antibody level-it suggests vigilance without premature judgment. By framing the 0.2 reading as both a diagnostic compass and a prompt for deeper inquiry, Edward champions a nuanced approach that respects variability across individuals and laboratories. This perspective encourages clinicians and patients alike to embrace complexity, ensuring early signals are neither overlooked nor over-interpreted but thoughtfully incorporated into holistic care.
Edward_Philips has masterfully articulated how an RNP antibody level of 0.2 transcends mere quantification to become a subtle yet pivotal biomarker in the complex landscape of autoimmune assessment. This commentary rightly emphasizes that such a low-level presence should not be hastily labeled as conclusive or dismissed outright. Instead, it serves as a crucial early alert-an invitation to integrate lab data with thorough clinical evaluation, including symptom review and patient history. The analogy of the “soft glow of twilight” is particularly evocative, capturing the level’s ambiguity and signaling a moment for heightened clinical vigilance without premature assumptions. This perspective realistically reflects the individualized nature of autoimmune diagnostics, where each antibody measurement must be interpreted within a broader, evolving clinical tapestry. Ultimately, Edward’s nuanced insight encourages a balanced approach-valuing subtle serological cues as guiding threads that lead toward comprehensive and personalized patient care.
Edward_Philips presents a profoundly insightful and nuanced perspective on the significance of an RNP antibody level of 0.2. This commentary beautifully underscores that such a value, while modest, is far from insignificant-it acts as an early signal inviting thorough clinical exploration rather than a definitive diagnostic endpoint. The metaphor of a “soft glow of twilight” elegantly captures the ambiguous yet meaningful nature of this finding, portraying it as a moment of cautious observation and potential early detection in autoimmune evaluation. Importantly, Edward highlights the critical interplay between laboratory variability, individual patient context, and the spectrum of autoimmune manifestations. This layered understanding encourages clinicians and patients alike to embrace complexity, fostering a personalized, integrative approach that values subtle serological clues as gateways to deeper inquiry and comprehensive care.
Edward_Philips masterfully conveys that an RNP antibody level of 0.2 is far more than a simple laboratory figure; it embodies the delicate threshold that invites careful clinical consideration. This commentary highlights not only the nuanced role such a value plays in the diagnosis of autoimmune diseases but also the inherent variability in serological testing and patient presentations. The eloquent metaphor of the “soft glow of twilight” poignantly encapsulates the ambiguity and cautious hope embedded in this finding-a subtle marker that prompts a broader, more individualized investigation rather than definitive conclusions. Edward’s insights reinforce the importance of integrating laboratory results with clinical context, underlining that autoimmune assessment is an evolving narrative requiring vigilance, personalized inquiry, and a multidimensional approach to truly untangle the complexities of immune function.
Edward_Philips’ exploration of the RNP antibody level at 0.2 eloquently highlights the intricate balance clinicians must strike when interpreting subtle serological findings. By framing this value as a “soft glow of twilight,” he captures the delicate threshold between normalcy and potential pathology, emphasizing that such measurements are not standalone verdicts but rather critical pieces in a larger diagnostic puzzle. This perspective reinforces the necessity of individualized patient assessment, where lab results are contextualized alongside clinical symptoms, history, and additional testing. The commentary also thoughtfully addresses laboratory variability and patient diversity, reminding us that immune function is a dynamic and highly personalized domain. Taken together, this nuanced viewpoint encourages both vigilance and prudence-prompting deeper inquiry while avoiding undue alarm, ultimately fostering a holistic, patient-centered approach to autoimmune evaluation and care.
Edward_Philips’ commentary on an RNP antibody level of 0.2 offers a compelling reflection on the intricacies of autoimmune diagnostics. His metaphor of the “soft glow of twilight” poignantly conveys the subtle but meaningful nature of this marker-not a conclusive diagnosis, but a nuanced signal warranting deeper clinical investigation. This perspective underscores the importance of contextualizing lab results within each patient’s unique clinical picture, acknowledging the variability between laboratories and individual immune responses. Importantly, the 0.2 value acts as an early alert rather than a verdict, prompting multidisciplinary assessment including symptom evaluation, further serological testing, and imaging when appropriate. Edward’s thoughtful analysis reminds clinicians and patients that autoimmune evaluation is an evolving, personalized journey, where seemingly modest antibody levels play a vital role in guiding comprehensive, patient-centered care without triggering undue alarm.
Edward_Philips eloquently captures how an RNP antibody level of 0.2 is far from a mere statistic; rather, it symbolizes an intricate interplay within the immune system that demands thoughtful interpretation. This subtle biomarker acts as a beacon signaling the need for comprehensive clinical evaluation while resisting premature conclusions. The metaphor of a “soft glow of twilight” beautifully conveys the nuance-indicating a borderline yet meaningful presence that invites deeper inquiry rather than definitive diagnosis. Edward’s emphasis on the variability across laboratories and diverse patient presentations reminds us to view this number not in isolation but as part of a complex clinical mosaic. Such a perspective underscores the importance of personalized medicine, advocating for a diligent, multifaceted approach that integrates serology, symptomatology, and patient history to truly understand the immune narrative behind this delicate finding.
Edward_Philips’ commentary enriches our grasp of an RNP antibody level at 0.2 by framing it as a nuanced indicator rather than a binary result. The depiction of this value as the “soft glow of twilight” elegantly conveys its role as a subtle but meaningful signal within a larger immune landscape. This level invites careful clinical scrutiny, urging clinicians not to jump to conclusions but to pursue a comprehensive and personalized assessment that integrates serology, patient history, and other diagnostic modalities. Moreover, Edward emphasizes the variability inherent in laboratory reference ranges and the diversity of patient presentations, underscoring that interpretation must be individualized. This balanced perspective reminds us that such antibody measurements serve as an early alert and important piece of the autoimmune puzzle, ultimately encouraging deeper inquiry and thoughtful management rather than premature labeling or undue concern.
Edward_Philips offers a profoundly insightful perspective on the significance of an RNP antibody level at 0.2, framing it as a subtle yet meaningful biomarker rather than a definitive diagnostic endpoint. His analogy of the “soft glow of twilight” beautifully captures the delicate balance between normal immune function and potential autoimmune activity, emphasizing that such a measurement serves as an early signal calling for further clinical exploration. By highlighting the variability across laboratories and individual patient presentations, Edward underscores the necessity of a nuanced, personalized approach to interpretation-one that goes beyond numerical values to incorporate clinical history, symptoms, and additional testing. This commentary is a compelling reminder that RNP antibody levels, especially those near borderline thresholds, weave into a broader, intricate narrative of immune health that demands vigilance, thoughtful inquiry, and a comprehensive, patient-centered strategy rather than premature conclusions or undue alarm.
Edward_Philips’ insightful reflection on an RNP antibody level of 0.2 beautifully conveys the complexity behind what might initially appear as a simple lab value. His metaphor of the “soft glow of twilight” elegantly illustrates this subtle measurement as a cautious signal-not a definitive diagnosis-inviting clinicians and patients alike to undertake a thoughtful, nuanced interpretation. As he highlights, the variability in laboratory reference ranges and individual patient responses demands personalized, comprehensive evaluation incorporating clinical history, additional tests, and close monitoring. This commentary enriches the discourse by reminding us that autoimmune diagnostics transcend numbers alone; rather, each value plays a role within a broader, dynamic clinical narrative. Edward’s approach promotes balanced vigilance, where the 0.2 reading guides further exploration without provoking unnecessary alarm, exemplifying the intricate artistry required in managing immune health.
Edward_Philips masterfully elucidates the nuanced significance of an RNP antibody level of 0.2, transforming what might initially seem like an inconspicuous figure into a powerful clinical clue embedded within the complexity of autoimmune assessment. His eloquent comparison to the “soft glow of twilight” perfectly encapsulates the subtlety of this biomarker-a threshold that neither confirms nor excludes disease but beckons thoughtful, individualized evaluation. The commentary astutely highlights the variability inherent in lab methods and patient presentations, emphasizing that such values must be integrated with broader clinical context, symptomatology, and additional investigations. By framing the 0.2 reading as both a cautionary signal and an invitation for deeper inquiry, Edward reinforces that autoimmune diagnostics thrive on a balance of vigilance and prudence, avoiding premature conclusions while encouraging a holistic, patient-centered approach. This perspective enriches our understanding of immune dynamics and the artistry in interpreting laboratory data.
Edward_Philips provides a compelling and poetic exploration of the significance behind an RNP antibody level of 0.2. His depiction elevates this seemingly modest value beyond raw data, illustrating it as a nuanced signal that commands careful interpretation within the broader clinical context. By likening the reading to the “soft glow of twilight,” Edward highlights the ambiguous and delicate threshold at which immune function may be shifting-neither conclusively normal nor definitively pathological. This perspective eloquently acknowledges the diverse patient presentations and varying laboratory standards that complicate straightforward conclusions. Importantly, his commentary reinforces that such a finding should serve as an impetus for continued assessment and vigilance, rather than premature diagnosis or dismissal. It underscores the artistry involved in autoimmune diagnostics, reminding clinicians and patients alike that values like 0.2 contribute meaningfully to an unfolding clinical narrative requiring personalized, holistic evaluation.