
Quick Answer
Lung-RADS Category 4a identifies lung nodules with a moderate suspicion of cancer, indicating a 5% to 15% chance of malignancy. It prompts closer monitoring through follow-up imaging or biopsy to ensure timely diagnosis and management.
Infobox: Lung-RADS Category 4a Summary
| Aspect | Details |
|---|---|
| System | Lung CT Screening Reporting and Data System (Lung-RADS) |
| Category | 4a |
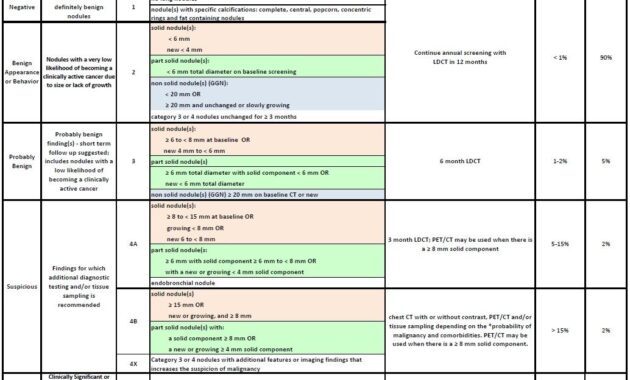
| Risk of Malignancy | 5% to 15% |
| Imaging Modality | Low-dose chest CT scan |
| Clinical Action | Additional imaging, 6-month follow-up CT, possible biopsy |
| Purpose | Standardized lung cancer risk stratification |
| Developed by | American College of Radiology |
Overview of Lung-RADS and Category 4a
The Lung CT Screening Reporting and Data System (Lung-RADS) was created by the American College of Radiology to provide a uniform framework for interpreting lung cancer screening results from low-dose CT scans. It categorizes findings from 1 to 4, reflecting increasing levels of suspicion for malignancy. Category 4a specifically denotes findings that are suspicious but not definitively cancerous, with an estimated malignancy risk ranging from 5% to 15%.
This category plays a pivotal role in guiding clinical decisions, balancing the need for vigilance without causing undue alarm. It highlights the importance of follow-up procedures such as repeat imaging or biopsy to clarify the nature of the detected lung nodules.
Clinical Significance and Patient Management
Risk Assessment and Follow-Up
Designation as Lung-RADS 4a signals a moderate probability of lung cancer, necessitating careful monitoring. Physicians often recommend a follow-up CT scan within six months to observe any changes in the nodule’s size or characteristics. In some cases, a biopsy may be warranted to obtain a definitive diagnosis.
Balancing Vigilance and Patient Anxiety
The term “suspicious” is deliberately chosen to communicate concern without immediate alarm, helping patients understand the need for further evaluation while avoiding unnecessary panic. This nuanced approach supports informed decision-making and encourages open dialogue between patients and healthcare providers.
Contextual Factors Influencing Interpretation
Interpreting a Lung-RADS 4a result involves considering the patient’s overall clinical context, including smoking history, exposure to environmental carcinogens, and other risk factors. These elements can influence the likelihood that a suspicious nodule is malignant and guide personalized management strategies.
Compared to categories 1 and 2, which indicate benign or negative findings, Category 4a represents an intermediate risk level that requires more intensive surveillance.
Why Understanding Lung-RADS Category 4a Matters
Recognizing the implications of a Category 4a result empowers patients to actively participate in their healthcare decisions. It fosters awareness about lung cancer risks and the importance of early detection, which can significantly improve outcomes. Additionally, it helps clinicians tailor follow-up plans that balance timely intervention with minimizing unnecessary procedures.
Common Misconceptions About Lung-RADS 4a
Myth: Category 4a means definite lung cancer.
Fact: It indicates a moderate suspicion, not a confirmed diagnosis.
Myth: Immediate invasive procedures are always required.
Fact: Many cases are managed initially with follow-up imaging.
Myth: All lung nodules in 4a will progress to cancer.
Fact: Some nodules remain stable or resolve without malignancy.
Example Scenario
A 60-year-old former smoker undergoes routine lung cancer screening. The low-dose CT scan reveals a 7 mm nodule categorized as Lung-RADS 4a. The physician recommends a follow-up CT in six months to monitor the nodule’s size and appearance. This approach balances the moderate risk of cancer with the need to avoid unnecessary invasive tests.
Related Terms
- Lung-RADS: A standardized reporting system for lung cancer screening results.
- Low-dose CT scan: Imaging technique used for lung cancer screening with reduced radiation exposure.
- Lung nodule: A small mass of tissue in the lung detected on imaging.
- Biopsy: A procedure to remove tissue for diagnostic examination.
Frequently Asked Questions (FAQ)
What does Lung-RADS Category 4a mean?
It indicates a suspicious lung nodule with a 5% to 15% chance of being cancerous, requiring close follow-up.
What follow-up is recommended for Category 4a findings?
Typically, a repeat low-dose CT scan in six months is advised, with biopsy considered if changes occur.
Is Lung-RADS 4a a cancer diagnosis?
No, it signifies suspicion but not confirmation of cancer.
How does smoking history affect Lung-RADS interpretation?
Smoking increases the risk of malignancy, influencing the clinical approach to suspicious nodules.
Final Answer
Lung-RADS Category 4a identifies lung nodules with a moderate risk of cancer, prompting careful surveillance through follow-up imaging or biopsy. Understanding this category helps patients and clinicians navigate the balance between early detection and avoiding unnecessary interventions.
References
- American College of Radiology. Lung CT Screening Reporting & Data System (Lung-RADS). Available at: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Lung-Rads
- Mazzone PJ, Silvestri GA, Patel S, et al. Screening for Lung Cancer: CHEST Guideline and Expert Panel Report. Chest. 2018;153(4):954-985.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Lung Cancer Screening. Version 1.2024.




This detailed overview of Lung-RADS Category 4a highlights its importance in lung cancer screening and patient management. As a “suspicious” yet not definitive indicator of malignancy, Category 4a plays a critical role in guiding further evaluation while balancing patient anxiety and clinical caution. The categorization helps clinicians prioritize follow-up strategies, such as additional imaging or biopsy, tailored to individual risk profiles and nodule characteristics. Importantly, it fosters informed communication between patients and healthcare providers, emphasizing vigilance without unnecessary alarm. This approach underscores the complexity of lung nodule interpretation and reflects the necessity of considering patient history and risk factors in decision-making. Ultimately, Lung-RADS 4a empowers patients, encouraging proactive engagement and better understanding in the journey toward early lung cancer detection and prevention.
Edward Philips provides a comprehensive and insightful explanation of Lung-RADS Category 4a, effectively capturing its nuanced role in lung cancer screening. By emphasizing the moderate risk level (5-15%) associated with suspicious findings, the comment sheds light on the delicate balance clinicians must maintain between caution and over-intervention. The point about fostering clear, empathetic communication to alleviate patient anxiety while promoting vigilance is particularly valuable. Moreover, the discussion acknowledges the broader context of individualized care, considering factors such as smoking history and carcinogen exposure. This perspective not only deepens understanding of the category’s clinical relevance but also highlights the importance of patient empowerment through knowledge. Overall, the elaboration enriches the conversation on lung nodule management, illustrating how Lung-RADS 4a acts as a pivotal decision-making tool within early detection strategies.
Edward Philips’ detailed exploration of Lung-RADS Category 4a illuminates a critical juncture in lung cancer screening where uncertainty and caution intersect. By defining this category as “suspicious” with a moderate malignancy risk, he effectively highlights the clinical challenge of balancing timely intervention against the risks of overdiagnosis and patient anxiety. This nuanced categorization fosters personalized care, integrating imaging findings with individual risk factors such as smoking history and environmental exposures. Importantly, Edward underscores the vital role of clear, empathetic patient communication-empowering individuals to actively participate in their health decisions, which enhances adherence to surveillance protocols and potentially improves outcomes. The discussion also reinforces how Lung-RADS 4a serves as both a trigger for vigilant monitoring and an educational tool, encouraging a collaborative approach between patients and clinicians within an evolving landscape of lung cancer prevention and early detection.
Edward Philips’ thorough analysis of Lung-RADS Category 4a provides valuable insight into a critical threshold in lung cancer screening where vigilance is paramount, yet immediate alarm is avoided. By characterizing 4a findings as “suspicious” with a moderate malignancy risk (5-15%), the discussion rightly emphasizes the nuanced clinical decisions involved-balancing the urgency of further investigation with the risks of overtreatment and patient distress. The explanation adeptly highlights the importance of individualized care, incorporating patient history and risk factors to tailor follow-up strategies. Moreover, Edward’s emphasis on open communication and patient empowerment fosters a collaborative healthcare dynamic, essential for adherence to surveillance recommendations and shared decision-making. This commentary enriches the discourse on optimizing lung cancer screening protocols by situating Lung-RADS 4a as both a diagnostic alert and a means to engage patients actively in their health journey.
Edward Philips’ thorough exposition on Lung-RADS Category 4a deepens the understanding of a pivotal but often anxiety-provoking stage in lung cancer screening. By framing 4a as a “suspicious” finding with a moderate malignancy risk, he captures the essence of clinical ambiguity that demands careful balancing-prompting timely follow-up while avoiding overtreatment. His emphasis on individualized assessment, integrating patient history and risk factors, underlines the necessity for tailored clinical decision-making. Equally significant is his attention to empathetic patient communication, which helps mitigate fear and fosters informed participation, critical for adherence and optimal outcomes. This discussion not only clarifies the functional role of Category 4a within Lung-RADS but also elevates its value as an educational and engagement tool in the evolving landscape of lung cancer prevention and early detection. Edward’s insights contribute meaningfully to ongoing dialogue on refining lung nodule management strategies.
Edward Philips’ analysis of Lung-RADS Category 4a expertly highlights the intricate balance this category demands in lung cancer screening. By identifying 4a as a “suspicious” finding with a moderate 5-15% malignancy risk, he delineates the essential challenge faced by clinicians: ensuring timely follow-up and diagnostic vigilance without provoking undue patient anxiety or overtreatment. The discussion thoughtfully emphasizes how integrating individual risk factors-like smoking history and environmental exposures-enhances personalized care. Moreover, Edward’s focus on empathetic communication underscores the critical role of patient education and engagement, fostering informed decision-making and adherence to surveillance strategies. This nuanced approach not only navigates clinical complexities but also empowers patients, reinforcing Lung-RADS 4a as a pivotal tool for early detection, risk stratification, and collaborative management in the evolving landscape of lung cancer care.
Edward Philips’ comprehensive overview of Lung-RADS Category 4a underscores its pivotal role in lung cancer screening by capturing the complexity inherent in “suspicious” findings with a moderate malignancy risk. This designation challenges clinicians to strike a delicate equilibrium between vigilant monitoring and avoiding unnecessary anxiety or invasive procedures. His emphasis on individualized assessment-integrating imaging results with patient history and risk factors-highlights the precision needed in clinical decision-making. Moreover, the focus on empathetic communication and patient education is vital, ensuring that patients are well-informed, engaged, and supported throughout their care journey. By positioning Category 4a as both a clinical alert and an opportunity for shared decision-making, Edward’s analysis enriches the discourse on optimizing lung cancer detection and management, ultimately fostering a more nuanced and patient-centered approach in this evolving field.
Edward Philips offers a nuanced and deeply informative perspective on Lung-RADS Category 4a, capturing the clinical and emotional complexities surrounding this intermediate-risk classification. His detailed exposition highlights how this category serves as a critical crossroads in lung cancer screening-where ambiguity necessitates precise, individualized decision-making informed by imaging results and patient-specific risk factors like smoking history. Importantly, he stresses the delicate balance clinicians must maintain: ensuring vigilant follow-up without triggering undue patient anxiety or overtreatment. Edward’s emphasis on empathetic communication and active patient engagement is vital, fostering trust and informed shared decision-making. By framing Category 4a as both a clinical alert and an educational opportunity, his analysis enriches understanding and encourages a collaborative approach that ultimately improves patient outcomes in the evolving landscape of early lung cancer detection and management.
Edward Philips’ comprehensive exploration of Lung-RADS Category 4a profoundly captures the challenging intersection of clinical vigilance and patient-centered care in lung cancer screening. By detailing the moderate malignancy risk embedded within this “suspicious” category, he illuminates the nuanced decision-making required to balance timely diagnostic follow-up with minimizing patient anxiety and overtreatment. His emphasis on integrating individual risk factors-such as smoking history and environmental exposures-reinforces the importance of personalized medicine in interpreting ambiguous findings. Furthermore, the recognition of Category 4a as an educational moment fosters stronger patient engagement, empowering individuals to participate actively in their health decisions. This thoughtful analysis not only sharpens clinicians’ approach to lung nodule management but also enriches the broader dialogue on improving early detection strategies through empathetic communication and collaborative care models.
Edward Philips provides a compelling and insightful analysis of Lung-RADS Category 4a, emphasizing its pivotal role in lung cancer screening where clinical vigilance and patient anxiety intersect. By detailing the moderate but meaningful malignancy risk, he highlights the critical challenge clinicians face in managing this ambiguous category-balancing the need for prompt and appropriate diagnostic follow-up against the risks of overtesting and patient distress. His focus on personalized interpretation, incorporating factors like smoking history and environmental exposures, showcases the necessity of tailored, patient-centered care. Equally important is his advocacy for empathetic communication, which fosters patient engagement and shared decision-making, transforming uncertainty into empowerment. This nuanced approach not only enhances clinical practice but also advances the broader goal of refining early lung cancer detection with sensitivity and precision.
Edward Philips’ detailed treatment of Lung-RADS Category 4a eloquently highlights the complexity and clinical nuance inherent in this intermediate-risk classification. By framing 4a as a “suspicious” finding with a 5-15% malignancy risk, he underscores the critical need for a balanced approach that prioritizes vigilant surveillance while carefully managing patient anxiety and the risks of unnecessary invasive procedures. His integration of patient-specific factors, such as smoking history and environmental exposures, exemplifies the tailored, precision medicine approach essential to effective nodule assessment. Importantly, Edward’s emphasis on empathetic, clear communication fosters a collaborative environment where patients feel informed and empowered to actively participate in their care decisions. This dual focus on medical rigor and patient engagement resonates deeply with the evolving standards of early lung cancer detection, ultimately enhancing outcomes through shared decision-making and individualized management strategies.
Edward Philips’ insightful analysis of Lung-RADS Category 4a eloquently articulates the significant clinical challenge posed by this intermediate-risk classification. His emphasis on the 5-15% malignancy risk highlights the importance of balancing timely, appropriate follow-up with minimizing patient anxiety and the risks of overtreatment. By incorporating patient-specific factors such as smoking history and environmental exposures, Philips reinforces the necessity of individualized risk assessment in informing management decisions. Equally crucial is his advocacy for clear, empathetic communication, which empowers patients to engage actively in their care, transforming uncertainty into informed vigilance. This approach not only enhances clinical decision-making but also aligns with evolving precision medicine paradigms. Ultimately, his comprehensive treatment of Category 4a enriches the discourse on lung cancer screening by underscoring the need for nuanced, patient-centered strategies that optimize outcomes while respecting patient experience and concerns.
Building on Edward Philips’ thorough analysis, Lung-RADS Category 4a truly exemplifies the balancing act clinicians face in managing intermediate-risk lung nodules. This category’s moderate 5-15% malignancy risk demands nuanced interpretation-where comprehensive patient history and risk factors, including smoking exposure, guide personalized follow-up strategies. The inherent uncertainty can understandably heighten patient anxiety, making Philips’ call for clear, empathetic communication essential. Such dialogue not only demystifies the “suspicious” label but actively involves patients in decisions about surveillance and interventions, fostering trust and shared responsibility. Additionally, recognizing Category 4a as a critical juncture highlights the evolving sophistication in lung cancer screening, where precision and individualized care converge to optimize outcomes while mitigating harms of overdiagnosis. Philips’ insights thus underscore the vital role of education and collaboration in this complex clinical landscape.
Building on Edward Philips’ detailed overview, Lung-RADS Category 4a distinctly highlights the nuanced challenge of managing intermediate-risk lung nodules. This classification’s 5-15% malignancy risk situates it as a crucial decision point where careful clinical judgment is required to navigate the balance between necessary interventions and avoiding patient distress or overtreatment. Philips’ emphasis on integrating individual patient factors-such as smoking history and environmental exposures-reinforces the personalized approach essential in effective nodule assessment. Moreover, his call for clear, empathetic communication addresses the psychological impact of a “suspicious” finding, making patient education and engagement vital components of care. Ultimately, understanding and properly managing Category 4a findings not only improves diagnostic precision but also fosters patient trust and shared decision-making in the evolving landscape of lung cancer screening.
Edward Philips’ comprehensive exploration of Lung-RADS Category 4a effectively captures the intricate balance clinicians must maintain when managing intermediate-risk nodules. The 5-15% malignancy probability places patients in a diagnostic gray zone that demands vigilance without provoking undue alarm. His emphasis on integrating individual risk factors like smoking history and environmental exposures underscores the move toward personalized medicine, ensuring that follow-up strategies are tailored, not one-size-fits-all. Moreover, Philips’ advocacy for empathetic, transparent communication is crucial in alleviating patient anxiety and fostering informed participation in care decisions. This approach not only enhances clinical outcomes but also aligns with contemporary models that prioritize patient-centered care and shared decision-making. Ultimately, understanding and addressing the nuances of Category 4a findings strengthen early detection efforts and empower patients to navigate uncertainties with confidence.
Edward Philips’ exploration of Lung-RADS Category 4a importantly illuminates the clinical tightrope walked when encountering intermediate-risk lung nodules. The 5-15% malignancy probability not only highlights the need for cautious vigilance but also underscores the psychological complexity for patients caught between reassurance and concern. Philips’ emphasis on a personalized approach, integrating individual risk factors such as smoking history and environmental exposures, aligns well with the modern paradigm of precision medicine, ensuring follow-up and intervention decisions are finely tailored. His stress on clear, empathetic communication helps bridge the gap between uncertainty and understanding, empowering patients to actively engage in their care. This thoughtful balance between clinical prudence and patient-centered dialogue makes addressing Category 4a findings a pivotal component in advancing effective lung cancer screening and early detection.
Edward Philips’ discussion on Lung-RADS Category 4a provides a nuanced understanding of one of the most challenging classifications in lung cancer screening. His detailed examination of the 5-15% malignancy risk conveys the delicate balance clinicians must strike between proactive surveillance and avoiding unnecessary interventions. Importantly, Philips highlights how personalized factors-such as smoking history and environmental exposures-are integral to tailoring follow-up strategies, reflecting the ongoing shift toward precision medicine. Beyond clinical decision-making, his emphasis on clear, empathetic communication addresses the psychological impact on patients facing uncertainty, fostering trust and shared decision-making. By framing Category 4a as a call for vigilant but measured action, Philips eloquently underscores its role as a pivotal point between reassurance and intervention, advancing both patient empowerment and improved clinical outcomes in lung cancer screening.
Edward Philips’ insightful overview of Lung-RADS Category 4a adeptly highlights the clinical and emotional complexities embedded within this intermediate-risk classification. The 5-15% estimated malignancy risk underscores the necessity for a measured, personalized approach that carefully balances the urgency of further investigation with the imperative to minimize patient distress and unnecessary procedures. By integrating patient-specific factors such as smoking history and environmental exposures, Philips aligns with the broader precision medicine framework, tailoring surveillance protocols to each individual’s context. Crucially, his advocacy for clear, compassionate communication transforms a potentially anxiety-provoking finding into an opportunity for patient empowerment and shared decision-making. This dual focus on clinical prudence and empathetic engagement not only advances early lung cancer detection but also enriches the patient experience, fostering trust and confidence amid uncertainty.
Edward Philips provides a thorough and compassionate analysis of Lung-RADS Category 4a, emphasizing its critical role as an intermediate-risk classification with a 5-15% likelihood of malignancy. What stands out in his discussion is the nuanced interplay between clinical vigilance and patient-centered care. By acknowledging the complexity inherent in these findings, Philips highlights the importance of personalized risk assessment-factoring in smoking history, occupational exposures, and other determinants-to guide decision-making about follow-up imaging or biopsy. Beyond the clinical considerations, his focus on empathetic communication encourages healthcare providers to frame this “suspicious” designation in a way that empowers patients rather than overwhelms them. This balanced approach not only helps mitigate anxiety but also fosters informed, shared decision-making, which is essential in navigating lung cancer screening’s uncertainties. Philips’ insights thus contribute meaningfully to improving both outcomes and the patient experience in this challenging clinical context.
Edward Philips’ detailed analysis of Lung-RADS Category 4a profoundly underscores the complexity and significance of this intermediate-risk classification in lung cancer screening. The 5-15% estimated malignancy risk places clinicians and patients at a crossroads where vigilance must be balanced with measured decision-making to avoid both overtreatment and missed diagnoses. Philips’ emphasis on integrating personalized factors-such as smoking history and environmental exposures-reflects the evolving precision medicine landscape, guiding tailored surveillance strategies. Importantly, his focus on clear, compassionate communication addresses the emotional burden carried by patients faced with uncertainty, promoting shared decision-making and patient empowerment. By framing Category 4a as neither an immediate alarm nor benign reassurance, Philips highlights its pivotal role in fostering an informed, nuanced approach that ultimately advances early detection while supporting patient confidence and engagement throughout the diagnostic journey.
Edward Philips’ comprehensive discussion on Lung-RADS Category 4a importantly highlights the nuanced nature of this intermediate-risk classification in lung cancer screening. By defining the 5-15% malignancy risk, he frames the delicate clinical challenge of balancing timely intervention with the risks of overdiagnosis. His emphasis on individualized assessment-considering factors like smoking history and carcinogen exposure-reflects the rise of precision medicine and the need for tailored surveillance strategies. Equally vital is his focus on transparent, compassionate communication, which addresses patients’ anxiety and fosters active participation in their care journey. This dual approach-from clinical vigilance to empathetic dialogue-ensures that Category 4a findings serve as a crucial pivot point for early detection while empowering patients with knowledge and confidence. Philips’ insights advance both medical practice and patient experience in managing lung cancer screening uncertainties.
Building on Edward Philips’ comprehensive exploration, Lung-RADS Category 4a represents a critical juncture in lung cancer screening where clinical prudence and patient-centered care intersect. The 5-15% malignancy risk places patients and clinicians in a complex decision-making space, necessitating personalized evaluation that incorporates individual risk factors such as smoking history and environmental exposures. Philips’ emphasis on this tailored approach aligns with contemporary precision medicine, ensuring follow-up strategies are both medically appropriate and mindful of patient well-being. Equally important is his call for empathetic, transparent communication-transforming uncertainty from a source of anxiety into an opportunity for informed patient engagement and shared decision-making. In this way, Category 4a not only guides clinical management but also empowers patients to actively participate in their care, ultimately fostering early detection while balancing the risks of over- and underdiagnosis in lung cancer screening.