
Quick Answer
“Full code” is a medical directive indicating that all possible resuscitation measures, such as CPR and intubation, will be performed if a patient’s heart or breathing stops. It reflects a patient’s or surrogate’s choice to pursue aggressive life-saving interventions during critical emergencies.
Infobox: Full Code Status at a Glance
| Term | Full Code |
|---|---|
| Definition | Authorization to perform all resuscitative efforts during cardiac or respiratory arrest |
| Common Interventions | CPR, defibrillation, intubation, advanced life support |
| Opposite Directive | Do Not Resuscitate (DNR) |
| Documentation | Advanced Directive, POLST, medical record |
| Decision Factors | Patient health, prognosis, personal values, age |
| Setting | Hospitals, emergency care |
Overview of Full Code Status
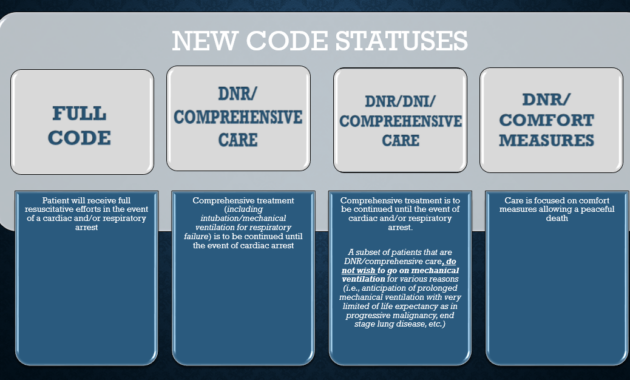
In hospital settings, the term “full code” designates a patient’s preference to receive comprehensive resuscitation efforts if they experience cardiac or respiratory arrest. This status authorizes healthcare providers to initiate all available life-saving procedures, including cardiopulmonary resuscitation (CPR), defibrillation, and airway management. It contrasts with a “Do Not Resuscitate” (DNR) order, which instructs medical staff to withhold such interventions.
Decision-Making and Patient Considerations
Choosing a full code status is a deeply personal decision influenced by multiple factors such as the patient’s age, overall health, prognosis, and individual values. Younger or healthier patients often opt for full resuscitation, anticipating a favorable recovery. Conversely, those with chronic illnesses or advanced age may prefer less aggressive approaches, prioritizing comfort over invasive treatments.
Healthcare professionals play a crucial role in facilitating informed discussions, explaining the procedures involved in resuscitation, potential outcomes, and the physical and emotional impacts. These conversations help align medical interventions with the patient’s goals and quality of life expectations.
Medical Context and Procedures
When a patient is designated as full code, this status is clearly documented in their medical records, often within an Advanced Directive or Physician Orders for Life-Sustaining Treatment (POLST). In emergencies, such as a “code blue” event indicating cardiac arrest, the medical team promptly initiates a coordinated resuscitation protocol.
Modern resuscitation techniques have evolved significantly, incorporating chest compressions, ventilations, automated external defibrillators (AEDs), and specialized medications. Despite technological advances, outcomes vary widely depending on the patient’s underlying health, the speed of intervention, and other situational factors.
Emotional and Ethical Dimensions
The decision to pursue full code status carries substantial emotional weight for patients and their families. The prospect of aggressive resuscitation can be both hopeful and distressing, as loved ones balance the desire to preserve life with the realities of illness progression.
Ethically, full code discussions extend beyond the mechanics of resuscitation to consider the quality of life post-intervention. For patients with advanced diseases, aggressive measures may not restore meaningful health, prompting difficult conversations about the benefits and burdens of continued treatment.
Healthcare System Implications
Full code orders also highlight broader challenges within healthcare systems, including resource allocation and cost considerations. High-intensity care demands significant hospital resources, raising questions about sustainability and the ethical distribution of medical interventions, especially when outcomes may be limited.
Alternatives to Full Code
Some patients may opt for a “partial code” status, which allows selective resuscitation measures while excluding others, such as avoiding intubation or chest compressions. This approach offers a middle ground, respecting patient autonomy and tailoring care to individual preferences and clinical realities.
Common Misunderstandings About Full Code
- Myth: Full code guarantees survival.
Fact: Resuscitation success depends on many factors and is not assured. - Myth: Full code means no limits on care.
Fact: Even full code patients may have other treatment limitations based on their condition. - Myth: Only patients can decide code status.
Fact: Surrogates or legal representatives may make decisions if patients lack capacity.
Example Scenario
Consider a 45-year-old patient admitted after a traumatic injury who is otherwise healthy. They choose full code status, indicating they want all resuscitative efforts if their heart stops. This decision reflects their hope for recovery and willingness to undergo aggressive treatment despite the risks involved.
Related Terms
- Do Not Resuscitate (DNR): A directive to withhold resuscitation efforts.
- Advanced Directive: Legal documents outlining a patient’s healthcare preferences.
- Physician Orders for Life-Sustaining Treatment (POLST): Medical orders reflecting patient wishes regarding life-sustaining treatments.
- Code Blue: Hospital emergency code signaling cardiac or respiratory arrest.
Frequently Asked Questions (FAQ)
- What does “full code” mean in a hospital?
- It means the patient has requested all possible resuscitation measures if their heart or breathing stops.
- Can a full code status be changed?
- Yes, patients or their surrogates can revise code status at any time based on changing health or preferences.
- Is full code appropriate for all patients?
- Not necessarily; it depends on individual health, prognosis, and personal values.
- What happens during a code blue for a full code patient?
- The medical team initiates CPR, defibrillation, and other life-saving interventions immediately.
Final Answer
“Full code” is a critical medical directive authorizing comprehensive resuscitation efforts during life-threatening emergencies. It reflects a patient’s or surrogate’s choice to pursue all available interventions to sustain life, balancing medical possibilities with personal values and health status. Understanding this designation is essential for informed healthcare decisions and effective communication within hospital settings.
References
- American Heart Association. (2020). Advanced Cardiovascular Life Support (ACLS) Provider Manual.
- National Institute on Aging. (2021). Advance Care Planning: Healthcare Directives.
- Institute of Medicine. (2015). Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life.
- American Medical Association. (2022). Code Status and End-of-Life Care.



