
In the realm of healthcare, particularly in hospitals, the phrase “full code” appears frequently. However, its implications and significance are often clouded in ambiguity for those outside the medical arena. Understanding what “full code” means is essential for both patients and families as it embodies critical decisions regarding medical interventions in life-threatening situations. This article endeavors to elucidate the concept of “full code,” the context surrounding it, and the ramifications of such a designation within a hospital setting.
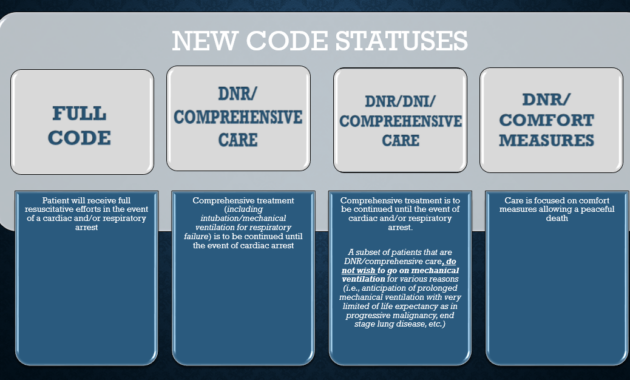
The term “full code” refers to a specific type of resuscitation directive given by a patient or, in some cases, a patient’s surrogate. It signifies that should a patient’s heart stop beating or they stop breathing, all resuscitation efforts will be initiated in an attempt to restore their life. This includes cardiopulmonary resuscitation (CPR), defibrillation, intubation, and advanced medical interventions. In contrast, a “do not resuscitate” (DNR) order indicates that no such efforts should be undertaken, reflecting the patient’s wishes or current health considerations.
Every patient’s circumstance is unique, and the decision to pursue a “full code” status involves numerous factors. Patients might choose this option based on their recovery expectations, overall health status, age, and personal values. For instance, a younger patient in relatively good health may opt for full resuscitation efforts, believing that the likelihood of recovery is favorable. Conversely, an elderly patient with multiple comorbidities might lean toward a more conservative approach, preferring to forgo aggressive measures in favor of comfort care.
This decision-making process is frequently accompanied by discussions among healthcare providers, patients, and their families. Clinicians are tasked with guiding these conversations by providing information on what full resuscitation entails, including potential outcomes and the physical and emotional toll of such interventions. Understanding the nuances of resuscitation can help patients make informed choices aligned with their values and life goals.
In the hospital environment, a “full code” status is documented in the patient’s medical record, often as part of an Advanced Directive or Physician Orders for Life-Sustaining Treatment (POLST). It is vital that medical teams are aware of a patient’s code status to ensure adherence to their wishes during emergencies. When a code blue is called—a hospital term for cardiac arrest—the healthcare team springs into action. If a “full code” is in effect, they are prepared to execute a multifaceted plan to resuscitate the patient.
The practice of resuscitation has evolved over time, with advancements in medical technology and techniques improving survival rates and outcomes. Chest compressions combined with ventilations, the use of automated external defibrillators (AEDs), and specialized medications are all components of modern CPR. However, it is critical to understand that while the intention behind a “full code” is to save a life, the process can often lead to varying outcomes based on the individual’s existing health conditions, the immediacy of medical response, and other situational factors.
The emotional weight of the decision surrounding “full code” status also cannot be understated. For families and loved ones, the prospect of enduring a resuscitation effort can be daunting. The tension between wanting to preserve life and facing the reality of a patient’s declining health plays a significant role in these pivotal discussions. These conversations may sometimes be fraught with anxiety, yet they can also offer an opportunity for families to reflect on their loved ones’ perspectives and beliefs regarding life and death.
Ethically, determining a “full code” status prompts significant deliberations, particularly concerning the quality of life. It’s essential to discuss not merely the mechanics of resuscitation but also the potential long-term effects of aggressive interventions. For patients with advanced disease processes, returning to a baseline of health post-resuscitation may not be feasible. In such situations, healthcare providers and families must weigh the merits of continued aggressive treatment against the possible outcomes of diminished quality of life.
In a larger context, “full code” provisions can also shed light on the systematic challenges faced by hospitals and healthcare systems. The approach to resuscitation often intersects with discussions about healthcare equity, resource allocation, and the associated costs of extensive medical interventions. High-intensity care can strain hospital resources, raising questions about sustainability and ethics in providing care that may not serve patients’ best interests in the long term.
As we explore further, curiosity about alternatives to “full code” emerges. Patients may consider the “partial code” designation, which allows for some interventions (like medication or oxygen) while foregoing others (like intubation or chest compressions). This practice serves to balance a desire for personal autonomy with the wince-inducing realities of critical care. It highlights the importance of personalized care tailored to individual needs and wishes.
Ultimately, the term “full code” is more than a directive; it is a multifaceted concept steeped in medical, ethical, and emotional dimensions. Understanding its implications is crucial for patients and families as they navigate the complex landscape of healthcare. The choices surrounding resuscitation carry profound significance, mirroring deeper beliefs about life, death, and the essence of human dignity. As discussions about end-of-life care continue evolving, the perspectives surrounding “full code” status will undoubtedly play a pivotal role in shaping future healthcare practices.




