
Tuberculosis, a scourge that has stalked humanity for millennia, continues to demand vigilance, particularly within the hallowed halls of healthcare facilities. Why the sustained emphasis on TB testing for healthcare workers? The rationale extends beyond mere regulatory compliance; it delves into the intricate interplay between occupational hazard, public health responsibility, and the ethical imperative to safeguard both providers and patients.
Understanding the Landscape of Tuberculosis Transmission
The Airborne Nature of the Beast: Mycobacterium tuberculosis, the causative agent of TB, disseminates through the air via droplet nuclei expelled during coughing, sneezing, or even speaking. These microscopic particles, capable of remaining suspended for extended periods, pose a significant risk, especially in enclosed environments such as hospitals, clinics, and long-term care facilities.
Latency vs. Active Disease: Exposure to M. tuberculosis doesn’t automatically equate to active disease. In many instances, the immune system successfully contains the infection, resulting in latent TB infection (LTBI). Individuals with LTBI are asymptomatic and non-infectious, but harbor the potential for reactivation to active disease, particularly when immune function wanes.
The Vulnerable Population Paradox: Healthcare workers, by virtue of their profession, are disproportionately exposed to individuals with active TB. Paradoxically, the very individuals dedicated to healing are placed at heightened risk of contracting this debilitating illness. This vulnerability necessitates proactive measures to detect and manage TB infection.
Mandatory Screening: A Web of Regulations and Recommendations
Federal Guidance: While no single federal law mandates universal TB testing for all healthcare workers, organizations like the Centers for Disease Control and Prevention (CDC) provide comprehensive guidelines and recommendations that serve as the bedrock for institutional policies.
State and Local Mandates: The regulatory landscape varies considerably across states and municipalities. Some jurisdictions have enacted legislation requiring routine TB screening for healthcare personnel, while others rely on adherence to CDC recommendations.
Accreditation Standards: Healthcare facilities seeking accreditation from organizations such as The Joint Commission must demonstrate compliance with infection control standards, which invariably include protocols for TB screening and prevention.
Who Is Subject to Screening? Unpacking the Eligibility Criteria
Risk-Based Assessment: The cornerstone of contemporary TB control strategies lies in risk-based assessment. Rather than blanket screening, healthcare facilities should conduct thorough evaluations to identify individuals at elevated risk of TB exposure or infection.
Direct Patient Contact: Personnel who engage in direct patient care, including physicians, nurses, respiratory therapists, and technicians, represent a primary target group for TB screening programs. The frequency of screening should be commensurate with the level of exposure risk.
High-Risk Settings: Individuals working in specific areas, such as pulmonary clinics, emergency departments, and correctional facilities, may warrant more frequent screening due to the higher prevalence of TB in these environments.
New Hires and Volunteers: Pre-employment TB screening is a standard practice in many healthcare institutions. This allows for the identification of individuals with pre-existing TB infection and the implementation of appropriate management strategies.
International Travel and Exposure: Healthcare workers who have recently traveled to or worked in countries with a high burden of TB should undergo screening upon their return.
Known Exposure Events: In the event of a known exposure to an individual with active TB, all potentially exposed healthcare workers should be promptly screened, regardless of their routine screening schedule.
The Screening Process: From TST to IGRA
Tuberculin Skin Test (TST): The TST, also known as the Mantoux test, involves injecting a small amount of tuberculin under the skin and assessing the induration (a raised, hardened area) 48-72 hours later. A positive TST indicates prior exposure to M. tuberculosis but cannot differentiate between LTBI and active disease.
Interferon-Gamma Release Assays (IGRAs): IGRAs are blood tests that measure the immune system’s response to M. tuberculosis antigens. These tests, such as QuantiFERON-TB Gold Plus and T-SPOT.TB, offer several advantages over the TST, including a single-visit requirement and reduced risk of false-positive results in individuals who have received the BCG vaccine.
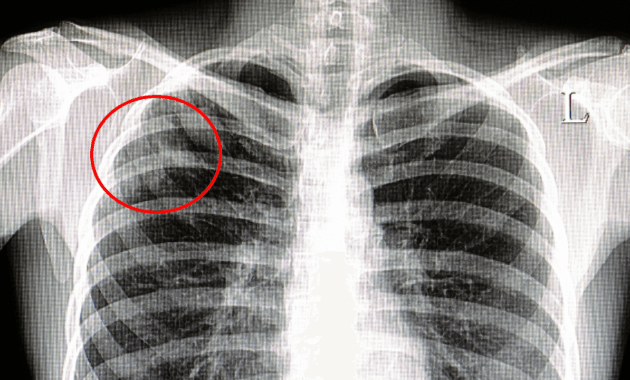
Follow-Up and Management: A positive TST or IGRA result necessitates further evaluation to rule out active TB disease. This typically involves a chest radiograph and clinical assessment. Individuals diagnosed with LTBI should be offered treatment to prevent progression to active disease.
Navigating the Ethical and Practical Considerations
Confidentiality and Privacy: Maintaining the confidentiality of TB screening results is paramount. Healthcare facilities must ensure that all information is handled in accordance with HIPAA regulations and other relevant privacy laws.
Addressing Stigma and Discrimination: TB carries a significant social stigma, which can deter individuals from seeking testing and treatment. Healthcare organizations must actively combat stigma and create a supportive environment for those affected by TB.
Resource Allocation: Implementing and maintaining a comprehensive TB screening program requires significant resources. Healthcare facilities must carefully allocate resources to ensure that screening is accessible, affordable, and effective.
The Evolving Landscape: The ongoing COVID-19 pandemic has underscored the importance of robust infection control practices in healthcare settings. The pandemic has also highlighted the potential for disruption of TB control efforts, necessitating renewed vigilance and adaptation of screening strategies.
In conclusion, the imperative to screen healthcare workers for tuberculosis stems from a confluence of factors: the inherent occupational hazard, the moral obligation to protect both caregivers and patients, and the overarching goal of safeguarding public health. While regulatory frameworks and screening methodologies may evolve, the fundamental principle remains constant: proactive TB control is essential for maintaining a safe and healthy healthcare environment. By embracing a risk-based approach, leveraging advanced diagnostic tools, and fostering a culture of vigilance, healthcare institutions can effectively mitigate the threat of TB and uphold their commitment to providing exemplary care.


