
Quick Answer
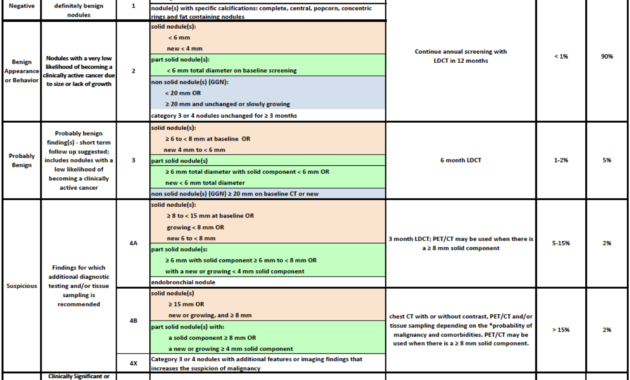
Lung-RADS Category 3 identifies lung nodules measuring 6 to 8 millimeters that are mildly suspicious but have a low malignancy risk (1-2%). It recommends a follow-up CT scan within six months to monitor any changes, balancing cautious observation with reassurance.
Infobox: Lung-RADS Category 3 Summary
| Aspect | Details |
|---|---|
| Category | Lung-RADS Category 3 |
| Nodule Size | 6-8 mm |
| Malignancy Risk | Approximately 1-2% |
| Recommended Action | Follow-up CT scan in 6 months |
| Purpose | Monitor nodule stability or progression |
| Common Patient Concern | Uncertainty and anxiety about cancer risk |
Overview of Lung-RADS and Category 3
The Lung Reporting and Data System (Lung-RADS) is a standardized classification tool designed to evaluate lung nodules detected on computed tomography (CT) scans. It helps radiologists and clinicians stratify the risk of lung cancer and guide subsequent management. Among its categories, Category 3 nodules are defined by their intermediate characteristics, typically nodules measuring between 6 and 8 millimeters in diameter that raise mild suspicion but are not overtly malignant.
Significance of Category 3 Nodules
Classifying a lung nodule as Category 3 signals the need for careful observation rather than immediate invasive procedures. Although the probability of cancer is low-estimated at 1 to 2 percent-these nodules warrant a follow-up CT scan within six months to detect any changes in size or appearance. This interval is critical for distinguishing stable benign nodules from those that may evolve and require further diagnostic intervention.
Why Monitoring Matters
Regular surveillance of Category 3 nodules is essential because lung nodules can behave unpredictably. Early detection of growth or morphological changes can significantly impact patient outcomes by enabling timely treatment. Conversely, stable nodules over time often indicate benignity, reducing unnecessary anxiety and invasive testing.
Factors Influencing Nodule Assessment
Not all lung nodules are identical in their biological behavior. Patient-specific factors such as age, smoking history, environmental exposures, and overall health influence the risk profile. Therefore, while a nodule may initially be categorized as Category 3, ongoing evaluation may adjust its risk classification based on new imaging findings or clinical context.
Common Misunderstandings About Lung-RADS Category 3
- Myth: Category 3 nodules are cancerous.
Fact: These nodules have a low malignancy risk and often remain stable. - Myth: Immediate biopsy is necessary.
Fact: Follow-up imaging is preferred before invasive procedures. - Myth: No follow-up is needed if the nodule is small.
Fact: Even small nodules require monitoring to detect changes.
Example Scenario
Consider a 60-year-old former smoker who undergoes a routine lung cancer screening CT scan. A 7 mm nodule is detected and classified as Lung-RADS Category 3. The physician recommends a follow-up CT in six months to monitor the nodule. Over this period, the nodule remains unchanged, providing reassurance and avoiding unnecessary invasive tests.
Related Terms
- Lung-RADS: A standardized lung nodule reporting system.
- Computed Tomography (CT): Imaging technique used to detect lung nodules.
- Lung Nodule: A small mass of tissue in the lung, often detected incidentally.
- Malignancy Risk: The probability that a nodule is cancerous.
- Follow-up Imaging: Repeat scans to monitor changes in nodules.
Frequently Asked Questions (FAQ)
- What does Lung-RADS Category 3 mean?
- It indicates a lung nodule with low suspicion for cancer, typically 6-8 mm in size, requiring follow-up imaging.
- How often should a Category 3 nodule be monitored?
- A follow-up CT scan is generally recommended within six months to assess for any changes.
- Is a biopsy needed for Category 3 nodules?
- Usually not immediately; biopsy is considered if the nodule grows or changes significantly.
- Can a Category 3 nodule become cancerous?
- While the risk is low, ongoing surveillance is important to detect any progression early.
- What factors affect the risk assessment of a lung nodule?
- Patient age, smoking history, nodule size, shape, and growth rate all influence risk evaluation.
Final Answer
Lung-RADS Category 3 identifies lung nodules that are mildly suspicious but carry a low risk of cancer, typically requiring a six-month follow-up CT scan. This approach balances vigilance with minimizing unnecessary invasive procedures, ensuring early detection of any changes while providing reassurance to patients.
References
- American College of Radiology. Lung-RADS Version 1.1. Available at: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Lung-Rads
- National Comprehensive Cancer Network. Lung Cancer Screening Guidelines. Available at: https://www.nccn.org/professionals/physician_gls/pdf/lung_screening.pdf
- MacMahon H, Naidich DP, Goo JM, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology. 2017;284(1):228-243.




This detailed explanation of Lung-RADS Category 3 effectively highlights its significance in lung nodule evaluation. It underscores that while nodules within this category may cause concern due to their size (6-8 mm), their low malignancy risk (1-2%) suggests that immediate invasive procedures are usually unnecessary. Instead, timely follow-up CT scans within six months play a critical role in monitoring any changes, balancing cautious vigilance with patient reassurance. The discussion also wisely emphasizes the individualized nature of risk, factoring in variables like smoking history and overall health, which can influence the nodule’s behavior. This framework helps both patients and clinicians navigate uncertainty, fostering informed decision-making and attentive surveillance that can ultimately guide appropriate care pathways.
Edward_Philips provides a comprehensive overview of Lung-RADS Category 3, effectively clarifying why this classification is both a source of concern and reassurance. The emphasis on the low malignancy risk (1-2%) coupled with the necessity for a six-month follow-up highlights the delicate balance between vigilance and avoiding unnecessary alarm. This category’s importance lies in its role as an early warning system, prompting careful monitoring rather than immediate intervention. Additionally, acknowledging patient-specific factors such as smoking history and overall health underscores how personalized assessments can refine risk stratification over time. By addressing the emotional and clinical complexities inherent in managing Category 3 nodules, the discussion encourages informed, patient-centered care that adapts to evolving imaging findings and changing risk profiles.
Edward_Philips offers an insightful and balanced exploration of Lung-RADS Category 3, clearly delineating its clinical implications and the rationale behind recommended follow-ups. By detailing the nodule size range (6-8 mm) and emphasizing the relatively low malignancy risk (1-2%), the explanation helps demystify what might initially provoke patient anxiety. Importantly, the focus on periodic reassessment through six-month interval CT scans illustrates how cautious surveillance serves as a prudent strategy to detect any early changes without resorting to invasive procedures prematurely. The nuanced perspective on how patient-specific factors-such as smoking history and overall health-can influence risk highlights the need for individualized care. Ultimately, this discussion underscores the delicate interplay between vigilance and reassurance, guiding both patients and clinicians through uncertainty with an approach that is both thorough and compassionate.
Edward_Philips thoughtfully captures the nuanced landscape of Lung-RADS Category 3, emphasizing its role as a pivotal juncture between watchful waiting and proactive intervention. The clear delineation of nodule size and malignancy risk offers essential clarity that can help alleviate patient anxiety while reinforcing the necessity of periodic imaging follow-ups. By highlighting the 1-2% likelihood of malignancy alongside the critical six-month reassessment interval, the commentary demonstrates how judicious monitoring serves as a key strategy to detect subtle changes early, reducing premature invasive procedures. Moreover, the acknowledgment of individual patient factors-such as smoking status and comorbidities-adds vital depth to risk assessment, underscoring the importance of personalized clinical judgment. Ultimately, this explanation balances caution with optimism, guiding both clinicians and patients through uncertainty with empathy and evidence-based precision.
Edward_Philips’s detailed exploration of Lung-RADS Category 3 adeptly conveys the fine balance between caution and reassurance integral to managing these lung nodules. By clearly defining the nodule size parameters (6-8 mm) and the associated low risk of malignancy (1-2%), the commentary helps mitigate undue patient anxiety while emphasizing the critical role of scheduled follow-up imaging at six months. This interval monitoring is a prudent clinical strategy that prioritizes early detection of any worrisome changes without resorting to unnecessary, invasive diagnostics. The thoughtful inclusion of individual risk modifiers-such as smoking history and comorbidities-underscores the importance of personalized care and flexible risk assessment. Ultimately, this comprehensive overview empowers both patients and healthcare providers to approach Category 3 nodules with informed vigilance, blending empathy with evidence-based precision to navigate uncertainty effectively.
Edward_Philips’s comprehensive explanation of Lung-RADS Category 3 provides valuable insight into the nuanced management of lung nodules that fall within this intermediate risk group. By defining the size criteria (6-8 mm) and clarifying the relatively low malignancy risk (1-2%), the discussion skillfully alleviates some patient anxiety while emphasizing the importance of scheduled six-month follow-up imaging. This approach underscores a prudent balance-avoiding premature invasive diagnostics while maintaining vigilant surveillance to detect any progression early. Moreover, highlighting variability in individual risk factors such as smoking history and overall health enriches the context, reinforcing that lung nodule assessment isn’t one-size-fits-all but tailored based on personalized information. Overall, the commentary thoughtfully navigates the challenging intersection of uncertainty and hope, equipping patients and providers with a clear framework to guide careful, evidence-based decision-making.
Edward_Philips’s thoughtful analysis of Lung-RADS Category 3 excellently highlights the delicate equilibrium between cautious monitoring and patient reassurance. By clearly defining the size parameters and emphasizing the low-but non-negligible-risk of malignancy, the commentary helps demystify what can be a daunting diagnosis for many patients. Importantly, the recommended six-month follow-up CT scan serves as a critical checkpoint to observe any nodule changes, illustrating a prudent, evidence-based approach that avoids unnecessary invasive interventions. The discussion also sensitively incorporates the variability of patient-specific factors, such as smoking history and comorbidities, which enrich the understanding that risk assessment is not static but personalized. Overall, this comprehensive perspective empowers both clinicians and patients to navigate the inherent uncertainty of Category 3 nodules with balanced vigilance and informed optimism.
Edward_Philips provides a nuanced and compassionate exploration of Lung-RADS Category 3, shedding light on its critical role in balancing vigilance with reassurance in lung nodule management. By defining the size parameters and clarifying the relatively low malignancy risk of 1-2%, the analysis effectively contextualizes the importance of timely six-month follow-up CT scans. This interval allows for careful monitoring of nodule stability or progression, minimizing unnecessary invasive interventions while ensuring early detection if malignancy develops. The emphasis on individualized risk assessment-factoring in smoking history and health status-acknowledges that no two nodules or patients are alike, highlighting the dynamic and personalized nature of care. This thoughtful commentary empowers both patients and healthcare providers to navigate the uncertainties of Category 3 nodules with informed caution and optimism.
Edward_Philips’s insightful breakdown of Lung-RADS Category 3 highlights the delicate interplay between cautious surveillance and patient reassurance in lung nodule management. By defining the 6-8 mm size range and emphasizing the relatively low malignancy risk of 1-2%, the commentary offers clarity that helps demystify this intermediate-risk category. The advocated six-month follow-up CT is a critical step, ensuring timely detection of any nodule changes while avoiding unnecessary invasive procedures. Importantly, the recognition that individual factors-such as smoking history and overall health-can influence risk reinforces that clinical decisions must be personalized rather than one-size-fits-all. This nuanced perspective empowers both patients and providers to navigate the uncertainty of Category 3 nodules with informed vigilance and balanced optimism, ultimately fostering better outcomes through ongoing, evidence-based monitoring.
Building upon Edward_Philips’s insightful explanation, this detailed overview of Lung-RADS Category 3 underscores the importance of a measured and personalized approach in managing these intermediate-risk lung nodules. The classification captures nodules measuring 6 to 8 millimeters with a low but tangible malignancy risk (1-2%), which situates patients in a delicate zone of watchful waiting rather than immediate intervention. The recommendation for a six-month follow-up CT scan exemplifies evidence-based prudence-balancing the need for vigilance with avoidance of unnecessary invasive procedures. Furthermore, considering individual patient factors such as smoking history and overall health status enriches clinical decision-making, highlighting that risk is not static but tailored to each patient’s context. This balanced perspective empowers both patients and clinicians to navigate the uncertainties with cautious optimism, ensuring dynamic monitoring and timely response to any changes, ultimately improving outcomes while minimizing anxiety.
Edward_Philips offers a clear and thoughtful explanation of Lung-RADS Category 3, emphasizing its role as an intermediate-risk classification that strikes a careful balance between reassurance and necessary vigilance. The identification of nodules sized 6 to 8 millimeters with a low malignancy risk (1-2%) highlights why a six-month follow-up CT is essential-not as an alarm but as a timely measure to monitor any changes in nodule behavior. Importantly, the commentary recognizes that this risk estimate is not absolute; patient-specific factors like smoking history and overall health influence the potential for malignancy and must guide personalized management. This approach helps mitigate patient anxiety by promoting an evidence-based, dynamic surveillance strategy that prioritizes safety while avoiding unnecessary invasive procedures. Ultimately, this insightful overview empowers both patients and clinicians to navigate uncertainty thoughtfully, making Lung-RADS Category 3 a pivotal step in managing lung nodules with cautious optimism.
Edward_Philips provides an excellent and comprehensive exploration of Lung-RADS Category 3, skillfully balancing the nuance of risk assessment with the patient experience. Emphasizing the 6 to 8 mm size range and the relatively low malignancy risk (1-2%) offers a reassuring perspective while underscoring the importance of the six-month follow-up CT to monitor for any subtle changes. This intermediate category serves as a reminder that lung nodules demand both vigilance and individualized evaluation, considering factors such as smoking history and overall health. The commentary thoughtfully addresses the emotional impact on patients by advocating ongoing surveillance without undue alarm, highlighting how this approach promotes timely detection and minimizes invasive procedures. Ultimately, this nuanced insight fosters a collaborative and informed dialogue between patients and clinicians navigating the complexity and uncertainties inherent in lung nodule management.