
Quick Answer
A borderline ECG indicates that the heart’s electrical activity shows minor irregularities that are neither clearly normal nor definitively abnormal. This ambiguous result often requires further clinical evaluation and monitoring to determine its significance and guide appropriate care.
Infobox: Borderline ECG at a Glance
| Term | Borderline ECG |
|---|---|
| Definition | Electrocardiogram results showing subtle deviations from normal heart electrical activity without clear pathology |
| Common Causes | Electrolyte imbalances, medication effects, anatomical variations |
| Clinical Significance | Requires further assessment; may indicate early or mild cardiac abnormalities |
| Next Steps | Additional testing (e.g., Holter monitor, echocardiogram), symptom evaluation, risk factor analysis |
| Interpretation | Dependent on clinical context and physician expertise |
Overview of Borderline ECG Findings
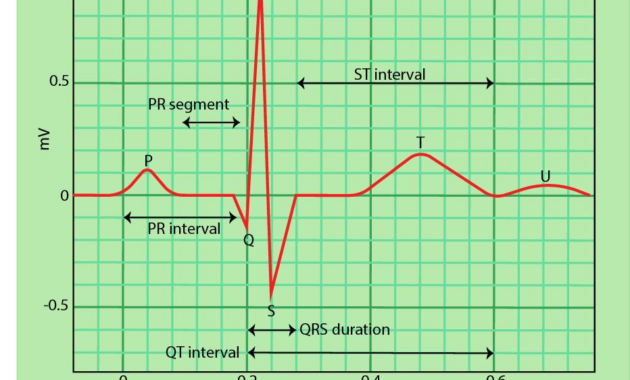
An electrocardiogram (ECG) records the heart’s electrical impulses, producing waveforms that reflect cardiac rhythm and function. When an ECG is described as “borderline,” it means the tracing exhibits slight abnormalities that do not clearly confirm or exclude heart disease. These subtle irregularities fall into a diagnostic gray zone, making interpretation challenging for clinicians and patients alike.
Such borderline results often arise from minor deviations in the ECG pattern that may be influenced by transient or non-cardiac factors. This ambiguity necessitates a comprehensive approach to patient evaluation rather than relying solely on the ECG reading.
Factors Contributing to Borderline ECG Results
Several elements can cause borderline ECG patterns, including:
- Electrolyte disturbances: Imbalances in potassium, calcium, or magnesium levels can alter cardiac electrical activity.
- Medications: Certain drugs may affect heart conduction and produce borderline changes.
- Anatomical variations: Structural differences such as mitral valve prolapse can influence ECG tracings.
These factors highlight the importance of considering the patient’s overall health status and potential reversible causes when interpreting borderline ECGs.
Clinical Context and Importance
Interpreting a borderline ECG requires integrating the patient’s medical history, presenting symptoms, and cardiovascular risk profile. For example, a borderline ECG in a patient experiencing chest discomfort or shortness of breath warrants more urgent and thorough investigation than in an asymptomatic individual.
Moreover, ECG interpretation is partly subjective and depends on the clinician’s expertise and the clinical environment. This variability underscores the need for careful clinical judgment and sometimes additional diagnostic tools.
Diagnostic Pathways Following a Borderline ECG
A borderline ECG often serves as a prompt for further diagnostic evaluation rather than a definitive conclusion. Common follow-up investigations include:
- Holter monitoring: Continuous ECG recording over 24-48 hours to detect intermittent arrhythmias.
- Echocardiography: Ultrasound imaging to assess cardiac structure and function.
- Laboratory tests: Checking electrolyte levels and other relevant biomarkers.
These additional assessments help clarify the clinical significance of borderline ECG findings and guide appropriate management strategies.
Why Borderline ECGs Matter
Borderline ECG results are clinically important because they may represent early signs of cardiac abnormalities or reversible conditions. Recognizing and investigating these subtle changes can prevent progression to more serious heart disease and improve patient outcomes through timely intervention.
Common Misconceptions About Borderline ECGs
Example Scenario
Consider a 45-year-old patient with mild fatigue and a borderline ECG showing slight T-wave abnormalities. Without other symptoms or risk factors, the physician may recommend electrolyte testing and repeat ECG monitoring. However, if the patient also reports chest pain, further cardiac imaging and specialist referral would be prudent to exclude ischemic heart disease.
Related Terms
- Electrocardiogram (ECG/EKG): A test that records the electrical activity of the heart.
- Holter Monitor: A portable device for continuous ECG recording over extended periods.
- Echocardiography: Ultrasound imaging of the heart’s structure and function.
- Hyperkalemia: Elevated potassium levels affecting cardiac conduction.
- Mitral Valve Prolapse: A structural heart condition that can influence ECG readings.
Frequently Asked Questions (FAQ)
- What does a borderline ECG mean for my heart health?
- It indicates minor irregularities that require further clinical evaluation to determine if they are benign or indicative of heart disease.
- Should I be worried if my ECG is borderline?
- Not necessarily, but it is important to follow up with your healthcare provider for additional tests and monitoring.
- Can medications cause borderline ECG results?
- Yes, certain medications can affect heart electrical activity and lead to borderline findings.
- What tests might follow a borderline ECG?
- Additional tests may include Holter monitoring, echocardiography, and blood tests to assess electrolytes and cardiac markers.
Final Answer
A borderline ECG reflects subtle deviations in heart electrical activity that are not clearly normal or abnormal. This ambiguous result necessitates a comprehensive clinical assessment, including patient history and further diagnostic testing, to determine its significance and guide appropriate management.
References
- Goldberger AL. Clinical Electrocardiography: A Simplified Approach. 9th ed. Elsevier; 2017.
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018;138(20):e618-e651.
- American Heart Association. Understanding Your ECG. Available at: https://www.heart.org/en/health-topics/heart-attack/diagnosing-a-heart-attack/understanding-your-ecg
- Wagner GS. Marriott’s Practical Electrocardiography. 12th ed. Lippincott Williams & Wilkins; 2014.



