
Quick Answer
Lung-RADS Category 4a marks nodules with a moderate cancer risk (about 5-15%). It prompts further evaluation, usually a high‑resolution CT follow‑up at 6-12 months, and may lead to biopsy depending on overall risk. The goal is early detection while minimizing unnecessary procedures.
Infobox
| System | Lung-RADS (Lung Cancer Reporting and Data System) |
|---|---|
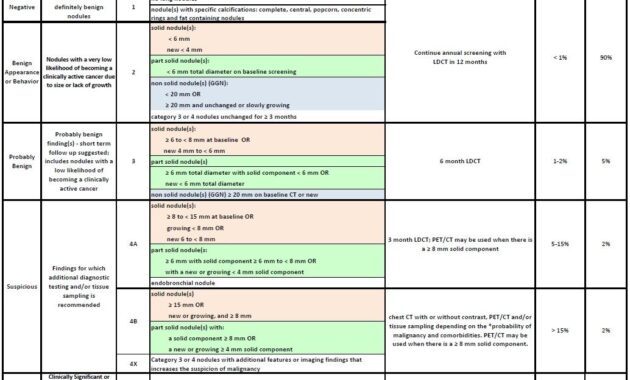
| Category | 4a |
| Definition | Nodules with moderate malignancy risk (roughly 5-15%) |
| Typical Features | Solid or Part‑solid nodules; commonly 6-8 mm; irregular or spiculated margins may raise concern |
| Follow‑up Guidance | High‑resolution CT at 6-12 months |
| Next Steps | Additional imaging and/or biopsy based on overall risk |
| Developer | American College of Radiology (ACR) |
| Target Population | Individuals undergoing LDCT screening for lung cancer |
Overview
Lung-RADS, short for Lung Cancer Reporting and Data System, is a framework designed to unify how lung imaging results from low-dose CT scans are described. It is primarily used in screening programs for people at elevated risk of lung cancer. Created by the American College of Radiology, Lung-RADS assigns nodules to distinct categories, each carrying different guidance for clinical management. Category 4a stands out for its nuanced implications in patient care.
Why It Matters
Understanding 4a helps clinicians balance vigilance with prudence. The designation signals a need for closer observation rather than an immediate diagnosis, guiding follow-up imaging and risk assessment. This approach supports early detection while potentially reducing unnecessary interventions for nodules that may be benign.
Common Misunderstandings
- Misconception: Category 4a means cancer is certain. Reality: It indicates a moderate risk (typically 5-15%), not a diagnosis.
- Misconception: All 4a nodules require an immediate biopsy. Reality: Biopsy decisions depend on overall risk, imaging evolution, and clinical judgment.
- Misconception: 4a only applies to smokers. Reality: While smoking is a major risk factor, 4a can occur in others with nodules of concern identified on LDCT.
Example
Consider a 65-year-old former smoker who undergoes routine LDCT. A solitary solid nodule measures 7 mm and shows irregular margins. It is categorized as 4a, prompting a follow-up high‑resolution CT in about 9 months. If the nodule grows or develops suspicious features, a biopsy may be discussed.
Related Terms
- Low-Dose CT (LDCT)
- High-Resolution CT (HRCT)
- Spiculation
- Nodule morphology
- Biopsy
- Other Lung-RADS categories (1-3, 4b, 4x)
FAQ
- What does Lung-RADS Category 4a mean?
- It indicates a moderate likelihood of cancer for a detected nodule, guiding further imaging and evaluation.
- What happens after a 4a classification?
- Typically, a follow-up HRCT is scheduled in several months to monitor changes; biopsy may be considered based on risk and evolution.
- Is biopsy always required for 4a nodules?
- No. Biopsy is considered when imaging changes or other risk factors justify tissue diagnosis; otherwise, surveillance may continue.
- How is the cancer risk estimated?
- Risk is inferred from nodule size, solidity, margins, and growth pattern, in combination with patient factors like age and smoking history.
Final Answer
Category 4a in Lung-RADS denotes a nodular lesion with a moderate chance of malignancy, prompting structured follow-up imaging and risk evaluation. Through careful surveillance and multidisciplinary decision-making, clinicians aim to detect cancer early while avoiding unnecessary procedures.
References
- American College of Radiology (ACR). Lung-RADS Atlas (latest version).
- National Cancer Institute. Lung cancer screening with low-dose CT.
- U.S. Preventive Services Task Force (USPSTF). Recommendations on lung cancer screening.




This detailed overview of Lung-RADS Category 4a highlights its pivotal role in lung cancer screening and patient management. As a classification recognizing nodules with a moderate malignancy risk (5-15%), 4a serves as a crucial decision point, balancing vigilance with the avoidance of unnecessary invasive procedures. The systematic follow-up through high-resolution CT scans and incorporation of patient-specific risk factors allow for tailored care, optimizing early detection while minimizing patient anxiety. Importantly, the collaborative approach among healthcare providers ensures comprehensive evaluation and thoughtful communication, empowering patients throughout the diagnostic process. Continued refinement of Lung-RADS and imaging advancements promises to enhance accuracy and outcomes in lung cancer screening, reinforcing the value of this standardized system in clinical practice.
Edward Philips’ thorough explanation of Lung-RADS Category 4a effectively underscores its essential role in stratifying lung nodules with moderate malignancy risk. Recognizing nodules with a 5-15% probability of cancer, this category facilitates a balanced clinical approach that prioritizes vigilant surveillance without resorting prematurely to invasive diagnostics. The structured follow-up imaging protocol ensures timely detection of changes, while integrating patient-specific factors promotes personalized care decisions. Moreover, the emphasis on clear communication and patient education addresses the psychological impact of indeterminate findings, fostering trust and adherence to management plans. As lung cancer screening programs continue to evolve, the precision and consistency afforded by Lung-RADS 4a remain vital in optimizing early detection and improving patient outcomes through multidisciplinary collaboration.
Edward Philips provides a comprehensive and insightful breakdown of Lung-RADS Category 4a, emphasizing its importance in managing lung nodules with an intermediate malignancy risk. This category acts as a critical threshold where careful monitoring through scheduled high-resolution CT scans and detailed risk assessments guide clinical decisions, helping avoid unnecessary invasive procedures while maintaining vigilance. Philips aptly highlights how nuanced imaging features like nodule size and morphology interplay with patient-specific factors, such as smoking history and family background, to shape individualized care plans. Additionally, the focus on patient communication and education is vital, addressing the emotional challenges that often accompany uncertain findings and ensuring adherence to follow-up protocols. Overall, this detailed explanation reinforces Lung-RADS 4a as a key element in early lung cancer detection, where multidisciplinary collaboration and technological advancements can substantially improve patient outcomes.
Edward Philips provides an excellent, well-rounded explanation of Lung-RADS Category 4a, a critical classification in lung cancer screening that denotes nodules with a moderate 5-15% malignancy risk. By clearly detailing the role of follow-up high-resolution CT scans at 6-12 months and the cautious consideration of biopsy, Philips emphasizes a balanced approach-early cancer detection without overwhelming patients with unnecessary invasive tests. His inclusion of common misconceptions helps demystify what a 4a designation truly means for both clinicians and patients. Furthermore, contextualizing this category within the broader Lung-RADS framework highlights its significance in standardized care, enabling personalized decisions based on imaging features, patient history, and risk factors. This nuanced approach not only enhances diagnostic accuracy but also supports patient-centered communication and multidisciplinary collaboration, ultimately improving outcomes in lung cancer screening programs.
Edward Philips offers a clear and comprehensive summary of Lung-RADS Category 4a, a key classification in lung cancer screening that identifies nodules with a moderate malignancy risk of approximately 5-15%. His explanation underscores the importance of scheduled follow-up with high-resolution CT scans within 6-12 months, reflecting a cautious yet proactive approach to monitoring. By emphasizing that biopsy is not automatically required and depends on evolving imaging findings and overall patient risk, Philips highlights a thoughtful balance between early detection and avoiding unnecessary invasive procedures. The attention to common misconceptions further clarifies the clinical implications of this category for both practitioners and patients. Overall, this detailed overview illustrates how Lung-RADS 4a supports optimized, individualized care pathways and multidisciplinary collaboration, fostering early identification of malignancy while minimizing undue diagnostic burden.
Edward Philips has provided a well-articulated and nuanced explanation of Lung-RADS Category 4a, emphasizing its role in lung cancer screening as an intermediate-risk classification. This category captures nodules with a 5-15% chance of malignancy, signaling the need for close monitoring through high-resolution CT follow-up at 6 to 12 months. Philips thoughtfully addresses that while the risk warrants vigilance, it does not mandate immediate biopsy, highlighting the importance of integrating imaging changes, patient history, and clinical judgment into management decisions. By clarifying common misconceptions, this overview helps patients and clinicians alike better understand what a 4a designation truly means, reducing unnecessary anxiety and interventions. Overall, the content reinforces Lung-RADS 4a as a critical communication tool that supports early detection and risk stratification within lung cancer screening programs, promoting balanced, patient-centered care and multidisciplinary collaboration.
Edward Philips’ explanation of Lung-RADS Category 4a offers a well-rounded perspective on managing lung nodules with moderate malignancy risk. This category plays a pivotal role in lung cancer screening by identifying nodules with a 5-15% chance of being cancerous and recommending structured follow-up through high-resolution CT scans at 6-12 months. Importantly, Philips clarifies that a 4a designation does not mean cancer is confirmed nor that biopsy is immediately necessary; instead, decisions are guided by changes in imaging and overall risk factors. Highlighting typical nodule characteristics and addressing common misconceptions enhances understanding for both clinicians and patients, reducing anxiety and unnecessary interventions. By contextualizing 4a within the Lung-RADS system, the explanation underscores the balance between early detection and prudent clinical management, fostering personalized care and multidisciplinary collaboration to improve screening outcomes.