
Carotid ultrasound is an essential diagnostic tool used to assess the health and functionality of the carotid arteries, which are critical vessels that supply blood to the brain. One of the terms frequently encountered in this context is “CCA,” which stands for Common Carotid Artery. Understanding the significance and the implications of this term can be crucial for patients and healthcare professionals alike.
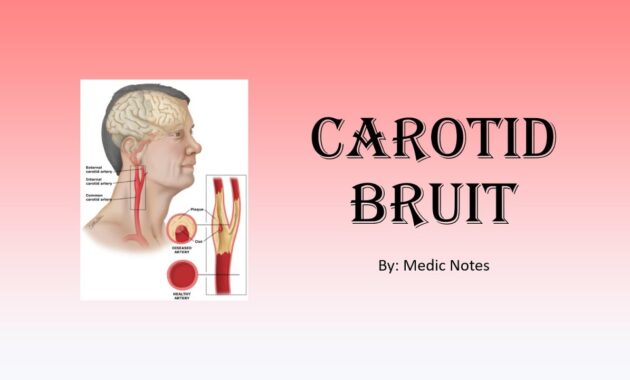
The common carotid artery bifurcates into two branches: the internal and external carotid arteries. The internal carotid artery primarily serves the brain, while the external carotid artery supplies blood to the face and neck. The CCA is the segment of the artery that is evaluated during carotid ultrasounds, making it a focal point in diagnosing cardiovascular health. Through this non-invasive imaging technique, professionals can obtain critical information about the structural and functional status of the CCA.
The first concern to address when discussing the CCA in carotid ultrasound is the procedure itself. During a carotid ultrasound, high-frequency sound waves are transmitted via a transducer placed on the neck, allowing for the visualization of blood flow and any potential abnormalities in the CCA. This painless, outpatient procedure typically lasts around 30 to 60 minutes, requiring minimal preparation. Patients are usually asked to lie down comfortably and may be instructed to turn their head in certain directions to enhance image capture.
The rationale behind assessing the CCA specifically lies in its susceptibility to atherosclerosis, a condition characterized by the buildup of plaque within the arterial walls. As plaque develops, it can lead to narrowing or stenosis of the artery, which significantly increases the risk of transient ischemic attacks (TIAs) or strokes. Identifying abnormalities in the CCA through regular ultrasounds serves as a preventive strategy against such serious cardiovascular events.
When interpreting carotid ultrasound results, several key measurements and observations target the CCA. These include assessing the intima-media thickness (IMT), evaluating the presence of plaque, and measuring blood flow velocities. The IMT refers to the thickness of the inner two layers of the carotid artery wall. An increased IMT can indicate an elevated risk of cardiovascular disease, prompting further evaluation or intervention. The presence of plaque can be classified based on its characteristics, such as echogenicity (brightness on the ultrasound), shape, and whether it is stable or unstable.
Additionally, blood flow velocity measurements taken during the ultrasound can reveal critical insights. High-velocity blood flow may indicate significant stenosis, while diminished velocities can suggest low blood flow secondary to blockage. Such evaluations are integral in determining treatment options, which may involve lifestyle modifications, medication, or in severe cases, surgical intervention.
Another important aspect to consider is the clinical guidelines surrounding the use of carotid ultrasound and the monitoring of the CCA. For individuals over a certain age or those with risk factors such as hypertension, diabetes, a family history of vascular diseases, or smoking, routine carotid ultrasound screenings may be advised. These guidelines aim to catch potential issues early, allowing for prompt management and reducing the risk of acute events.
For healthcare providers, understanding the implications of the CCA assessment is vital. Findings from carotid ultrasounds can inform treatment plans and encourage discussions with patients about lifestyle changes. For instance, patients diagnosed with increased IMT or plaque presence may be advised on dietary adjustments, exercise regimens, or medication to manage cholesterol and blood pressure, which ultimately addresses the underlying risk factors contributing to cardiovascular disease.
It is also crucial to discuss potential limitations of carotid ultrasound when evaluating the CCA. While it is an invaluable tool, it is not definitive. The accuracy of the ultrasound can sometimes be affected by factors such as patient obesity, calcified plaque, or operator expertise. Additionally, carotid ultrasound does not replace other diagnostic modalities such as angiography or MRI when a more comprehensive assessment is necessary. Understanding these nuances can assist patients in forming realistic expectations regarding their diagnoses and potential treatment outcomes.
In summary, the term CCA in the context of carotid ultrasound refers to the common carotid artery, a critical focus of this examination. The trial of understanding its significance poses a critical inquiry into a patient’s cardiovascular health. Through regular monitoring, healthcare professionals can assess the risk of cerebral vascular incidents, facilitate timely interventions, and ultimately contribute to improved health outcomes. As our population ages and the prevalence of vascular diseases escalates, recognizing the importance of the CCA in carotid ultrasound becomes increasingly relevant.
Involving patients in their healthcare journey through education about the CCA and its implications can foster better adherence to recommended screenings and lifestyle changes. Indeed, an informed patient is a powerful ally in the quest for optimal cardiovascular health.




